I decided to do my blog for this week on salivary gland stones since this is a common reason for soft tissue neck scans in our facility. I became interested in this after we scanned a young female who had a past history of salivary gland stones. She presented with pain and swelling in her left jaw. She told me a previous stone had been removed in her dentist’s office. The dentist used a small tweezers to remove it from the duct opening. The scan this time showed a very large stone in her duct. I wish I had an image but I can’t remember the patient’s name or when we scanned her. Anyhow, I doubt this stone was going to be removed easily!
Salivary gland stones are most common in the submandibular gland duct (75 - 80%) with the rest usually found in the parotid gland duct (25%). Stones are rare in the sublingual gland ducts. The stones are usually made up of calcium and can range in size from less than 1 mm to several centimeters. They are more common in males, after age 40, and some people are just more prone to developing them (just like some people are more prone to developing kidney stones). It is thought that stones form more commonly in the submandibular glands because the saliva found in these glands is thicker and has to drain uphill.
The symptoms of a salivary gland stone are pain and swelling in the jaw or face, or swelling of the gland itself. Another symptom is dry mouth. The symptoms are all more common at mealtimes. This is because the salivary glands produce extra saliva when you eat and the saliva doesn’t have anywhere to go because it is blocked by the stone. Infection and abscess can occur if the stone isn’t removed. Diagnosis can be by plain film x-ray, sialography, or CT.
Small stones at the duct opening can often be removed by a dentist. Endoscopy can be used to capture and remove stones using a dialator, basket or balloon. Open surgery is the last option. If stones recur in just one gland the individual gland can be removed and the mouth will still make enough saliva.
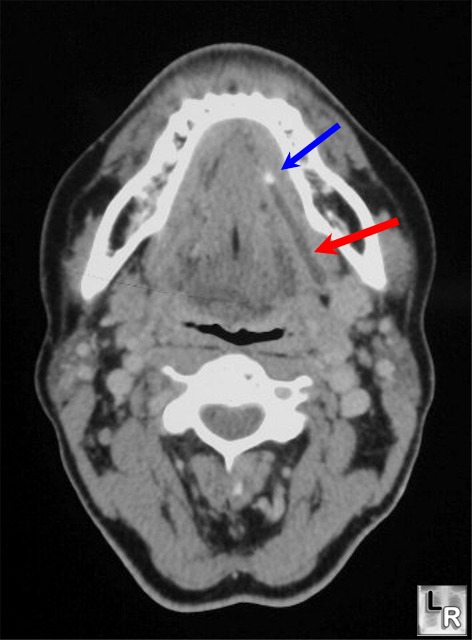
This CT image shows a stone in the submandibular duct (blue) and the dialated duct (red).
Image:
http://www.learningradiology.com/archives04/COW%20096-Sialolithiasis/sialolithcorrect.htm
References:
http://health.nytimes.com/health/guides/disease/salivary-duct-stones/overview.html
http://othn.iusm.iu.edu/salivaryglandendoscopy/
http://www.patient.co.uk/health/Salivary-Gland-Stones.htm


